

Breathing During Indoor Rowing
Don't just do it, do it well
Alison K. McConnell, BSc, MSc, PhD, FACSM, Professor of Applied Physiology, Centre for Sports Medicine & Human Performance, Brunel University
Introduction
As a student in the 1980s, I acquired two (at the time) rather unfashionable interests. The first was an interest in the physiology of breathing during exercise, and the second was rowing - the two interests were not unconnected. As a singularly ordinary rower, I was always let down the apparent inability of my breathing to keep pace with the demands of racing (or training for that matter). One of my crewmates once commented that I sounded as though someone had taken me by the throat at 500m and hadn't let go. I now know that I'm by no means unique in respect of my puffing and panting. Indeed, when we test rowers in the laboratory, the cardinal sign of impending exhaustion is a break-down of breathing discipline.
However, in common with all students of exercise physiology, I was taught that breathing presented no physiological limitation to human exercise performance (hence the unfashionable nature of my interest in it). This is because, the transport of oxygen to the muscles is not limited by its transfer through the lungs and into the blood. In other words maximal oxygen uptake (VO2max) is not limited by breathing. For many years I accepted the received wisdom that breathing doesn't limit exercise performance without a second thought. However, my personal (mostly excruciating) experience of competitive rowing led me to question what I had been taught. Eventually, I realised what I (and my teachers) had failed to appreciate - the limitations imposed by breathing need to be placed in a wider context than simply the supply of oxygen.
Breathing is a muscular process brought about by a group of muscles that are capable of demanding as much as 16% of available oxygen during maximal exercise1. This same group of muscles also act to stabilise the trunk, lower back and pelvis, and to transmit propulsive force during rowing. Hence, good breathing technique is at the very centre of good rowing technique. I'm pleased to say that in the 20 years since I initiated my (unfashionable) research on breathing and exercise, the area has moved from being unfashionable to being de rigeur. The work of breathing is now acknowledged to be a major limiting factor to exercise performance2, even in world-class athletes (perhaps more so). I hope this article will help to explain why respiratory limitations to exercise have achieved newfound credibility within sport science.
Later in this article, we'll look in more detail at the physiological limits imposed by breathing as well as the lesser know mechanical limitations. But before doing so, I want to explain a little about the physiology of the respiratory system, followed by some information about how breathing and rowing interact. In doing so, I will share with you the reasons why I believe that training your breathing muscles is every bit as important as squats, bench pulls and power cleans, in fact, more so.
Breathing: the fundamentals
At rest, we breathe approximately 15 times per minute, with a volume of around 0.5 litres (producing a 'minute ventilation' of 7.5 litres per minute [15 x 0.5]). The volume of each breath (tidal volume) depends on body size and metabolic rate (bigger people have larger lungs and take larger breaths, they also require more energy and oxygen to support their metabolism).
During heavy exercise, breathing frequency rises to around 40 to 50 breaths per minute. In the 'man in the street', tidal volume rises to around 3 to 4 litres (minute ventilation = 120 to 160 litres per minute), but in Olympic class oarsmen, tidal volume can be over 5 litres, resulting in minute ventilations of 250 to 300 litres per minute. Kilo for kilo, Olympic oarsmen have minute ventilations that are equivalent to thoroughbred racehorses!
We are all familiar with the act of breathing, which is a rhythmic pumping of the chest 'bellows' that sucks and in and out of the lungs. In order to breathe in, the volume of the chest cavity must increase in order to create a pressure gradient into which air moves. Increasing the thoracic volume momentarily creates a slightly negative pressure inside the lungs, which is equalised very rapidly by the movement of air into the lungs.
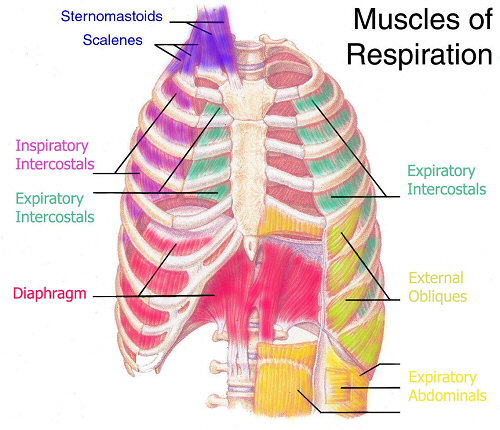
The 'physics' of this response are exactly the same as those behind a bicycle pump. To draw air into the pump you increase the volume of the pump by drawing the handle out; air flows into the pump to equalise the drop in pressure produced. When breathing out, the volume of the thoracic cavity must be reduced, thereby creating a slightly positive pressure that drives air out of the lungs. These changes in the volume of the thorax are brought about by the action of the breathing (respiratory) muscles (Figure 1).
The breathing muscles are divided into two sets; 1) the inspiratory muscles (diaphragm, inspiratory intercostals, sternomastoids, scalenes), and 2) the expiratory muscles (abdominals, external obliques, expiratory intercostals).
The action of the inspiratory muscles increases the volume of the chest cavity by lifting the rib cage upwards and outwards, and flattening the dome of the diaphragm and moving it downwards (like the handle of the bicycle pump being drawn out of the pump). The action of the expiratory muscles reduces thoracic volume by pulling the rib cage downwards and pushing the diaphragm up into the thoracic cavity.
The lungs and the chest wall (rib cage and associated structures) are elastic structures that naturally 'spring' back to their resting positions once the forces acting on them are removed. These forces are brought about by the breathing muscles, and to inhale, the inspiratory muscles must expand the thoracic compartment and stretch the lungs (this stores some elastic energy within the lung tissues). At the start on an inhalation, the inspiratory muscles are relaxed, and any elastic energy stored within the lungs and chest wall has been dissipated. Each intake of breath is therefore initiated from a point where all of the forces acting on the lung are in a state of balance.
When breathing at rest, only the inspiratory muscles are active. Inhalation occurs by contracting the inspiratory muscles, which inflates the lungs, causing them to stretch like a party balloon; to breathe out, all that is required is to relax the inspiratory muscles, and the lungs and chest wall spring back to their equilibrium position using stored elastic energy (like releasing an inflated party balloon).
During exercise, the rate and depth of breathing is increased, which requires the respiratory muscles to contract more forcefully, and quickly. The expiratory muscles begin to make a contribution to breathing during exercise, because the stored elastic energy from inspiration is not sufficient to achieve the expiratory flow rates required during exercise.
However, at all intensities of exercise the majority of the work of breathing is undertaken by the inspiratory muscles, because expiration is always assisted to some extent by stored elastic energy that was provided by the inspiratory muscles.
How breathing and rowing interact
Before discussing how breathing and rowing interact, its important to get a perspective on the unique 'animal' that is the world-class rower. In my view, it is no coincidence that rowers are renowned for the enormity of their lung capacity. The late Dr Mark Harries of the British Olympic Medical Centre once commented to Matthew Pinsent, 'My God man, you've got the lungs of a horse'. Sir Matthew's lung capacity is a whopping 8.25 litres, which is around 3 litres bigger than the 'average Joe', and 2 litres bigger than it should be for a man of his size. In his prime, his maximal oxygen uptake was around 8 litres per minute and his maximal ventilation around 300 litres per minute. Rowing a 2000m at ~460W, he respired approximately 1700 litres of air, and his inspiratory muscle power output was ~85W. The next time you're in the gym, dial up 85W on a cycle ergometer and see how this feels - it's a surprisingly large amount of work.
So what is it about having big lungs that is an advantage to a rower? I do not believe that it is because it gives them a greater VO2max, instead, I believe that having larger lungs enables rowers to maintain good breathing discipline during rowing. We'll consider this further in the section on the mechanical limitations imposed by breathing.
It has long been recognised that experienced rowers entrain their breathing to rowing stroke rate. Experienced rowers tend to confine their breathing to two main patterns; i) one expiration per drive and one inspiration during recovery (1:1), or ii) one complete breath during the drive and one complete breath during recovery (2:1). Research has shown that tidal volume (the volume of each breath) is constrained above a certain power output, with further increases in ventilation being brought about by increasing breathing frequency3. Some researchers have gone as far as to suggest that at high work rates, stroke rate may be dictated by the drive to breathe3, which reinforces the potent interrelationship of these two factors.
The linkage between stroke rate and breathing pushes the respiratory muscles to their limits. During a 2000m race, athletes commonly try to maintain the 2:1 breathing pattern; they breathe out during the initial part of the drive (when the blade is in the water), take a breath as they reach the end of the drive, breathe out again as they begin to come forward and take a small breath just before the 'catch'. This small breath at the catch is very important in terms of allowing the effective transmission of force from the stretcher to the blade handle (see 'Breathing related limitations to rowing: Mechanical').
In rowing, the same muscles that we use to breathe are also used for maintaining posture, 'core stability' and transmission of force during the drive phase of the stroke (see 'Breathing related limitations to rowing: Mechanical'). There are a number of critical points in the stroke where differing demands are placed upon the inspiratory muscles. At the finish, the hips are extended and the shoulders are behind the hips. This means that the muscles of the trunk must work against gravity to prevent the rower from falling backwards. At the same time, the rower needs to take a large, fast breath, which means that the inspiratory muscles are subjected to competing demands for postural stability and breathing. Once the rower reaches the catch, they must take another breath, but in this position, the movement of the diaphragm is impeded by the crouched body position. At the catch, the abdomen is compressed by the thighs pushing the liver, stomach and gut upwards against the diaphragm. This compression makes it harder for the diaphragm to contract, flatten and move downwards, as it must do in order to inflate the lungs. During the drive, the inspiratory muscles are subjected to competing demands for breathing, postural and force transmission. All in all, rowing places some varied and 'extreme' demands on the inspiratory muscles.
The combination of these demands renders the inspiratory muscles of rowers at heightened risk of becoming fatigued. Indeed, research has shown that the strength of the inspiratory muscles is 12-20% lower following a 2000m race4,5.
Most readers would agree that if fatigue is present in a group of muscles following a given task, these muscles are probably placing some limitation on the performance of that task. The earliest reports of breathing muscle fatigue following a competitive event appeared in the early 1980s, where significant declines in inspiratory muscle strength were observed following marathon running6. Later research confirmed these findings following marathon running7, but also provided data suggesting that ultra-marathon8 and triathlon9 competition were fatiguing to the respiratory system.
Under laboratory, and field-based research conditions, my own research group has also demonstrated inspiratory muscle fatigue following rowing4,5, cycling10 and swimming11, as well as a sprint triathlon12. This evidence of exercise-induced inspiratory muscle fatigue is probably the most compelling rationale for specific training of the inspiratory muscles. Readers who are interested in this topic are referred to the article on POWERbreathe® training by Eddie Fletcher in this section of the website.
Breathing related limitations to rowing: Mechanical
The mechanics of rowing are such that breathing must be entrained to stroke rate (see above). Failure to do so is not only uncomfortable, but also jeopardises the efficiency of the mechanical linkage between the blade handle and the major force producers of the lower body. In open class oarsmen, the forces driven from the stretcher, through the body and to the blade handle can be in the order of 900 Newtons (the weight of two bags of cement, or almost two hundred weight). Since the main force generators for the rowing stroke are located below the waist, if force is to be transmitted effectively to the blade handle, it must be transferred effectively through the trunk.
The diaphragm is the main inspiratory muscle, but it also plays an important role in postural control and the maintenance of intra-abdominal pressure (this is the pressure inside the abdominal compartment). Without an increase in intra-abdominal pressure when we lift objects, or exert force during a rowing stroke, the spine and pelvis are unstable. Under these conditions, the trunk flexes and fails to transmit the force generated by the lower body effectively to the object in our hands (be it a blade handle, or a suitcase). Why does this matter? Well consider the difference in mechanical efficiency of using a crow bar to lever something open compared with using a rod of metal that contains a number of loose joints. If the joints move, the force the rod transmits is lower, and its efficiency is reduced. The jointed rod in this analogy is your spine, and failure to maintain a stiff trunk reduces the efficiency of force transmission during the stroke. Central to generating this stiffness is the contraction of the diaphragm.
So what's this got to do with breathing? The pre-catch breath is important for maintaining the safe transmission of force, because the structural stability of the rib cage and lower back are affected by the pressures inside the chest and abdominal cavities, respectively. During the drive, the muscles of the trunk brace against the partially inflated lungs, allowing the internal pressures within the chest and abdomen to increase; this stiffens the trunk. Failure to maintain adequate internal pressures (because of an inadequate lung volume) may lead to an increased risk of rib stress factures and low back injury.
Furthermore, in an unpublished pilot study my research group has demonstrated that when the inspiratory muscles (including the diaphragm) are fatigued, the maximal static force generated at the catch is reduced. This suggests that the inspiratory muscles play a role in determining either the magnitude of the force generated by the lower body, or the efficiency of its transmission through the trunk, or both.
So we can see that the muscles of the trunk have a number of important roles during rowing, 1) contributing to the transmission of propulsive force, 2) maintaining structural stability of the spine and other bony structures, 3) breathing. However, these roles may become contradictory from time to time, which may impact negatively upon both performance and injury risk. Research has shown that when 'push comes to shove', the diaphragm's role in breathing takes precedence over its role in postural stability13. In other words, in situations of high ventilatory demand, such as exercise, the postural role of the inspiratory muscles is compromised, and it has been suggested that this may lead to an increased risk of injury due to spinal instability and a loss of postural control13. This means that when breathing discipline breaks down during rowing, the risk of injury increases, and performance is impaired.
What can we do to minimise these negative mechanical effects of breathing? A well-established method of increasing the fatigue resistance of any muscle is to resistance train it; stronger muscles work at lower relative intensities than weaker muscles, so their endurance and risk of fatigue are reduced. There is now good evidence that specific training of the inspiratory muscle using the POWERbreathe® improves performance in a range of sport, especially rowing4,5. For more information on this POWERbreathe® training see Eddie Fletcher's article on this section of the website.
Breathing related limitations to rowing: Physiological
We've considered the mechanical limitations posed by breathing during rowing, now I want to consider the physiological limitations. Fatigue of the inspiratory muscles is commonplace in many sports, but particularly so in rowing, where the muscles are subjected to multiple demands (see above). So what?
There are two very serious physiological repercussions of inspiratory muscle fatigue (IMF), and I will discuss each of these in turn:
- IMF increases breathing and whole body effort perception - makes you feel as though you are working harder
- IMF causes blood flow to the exercising limbs to be restricted - impairs oxygen delivery and metabolite removal from the working muscles
The underlying physiology is pretty straightforward; as a muscle fatigues, it requires a larger neural drive from the brain to activate the muscle fibres. The brain is very adept at judging the magnitude of the neural drive, and perceives an increase in the required drive as an increase in effort. Conversely, the magnitude of the neural drive to a muscle decreases after its strength has been improved by training.
After strength training, the brain perceives the decrease in neural drive as a reduction in effort. The inspiratory muscles interact with the brain in the same way as other muscles, so fatigue is associated with an increase in breathing effort14, and improvements in function after training are associated with a decrease in breathing effort4,15.
However, breathing effort also makes a big contribution to how hard the exercise feels as a whole, so reducing breathing effort also has a direct benefit upon whole body effort perception15.
Most people choose a pace that is just the right side of intolerable discomfort; in other words, we work as hard as is tolerable. So in the presence of IMF, the threshold of what is tolerable is reduced, which means a slower pace. Can anything be done to combat this? Yes, strengthening the inspiratory muscles with POWERbreathe® training prevents inspiratory muscle fatigue during rowing, which helps to stave off the escalating increase in effort as the race progresses4,10. POWERbreathe® training also reduces effort perception at any given power output. Thus, the limit of tolerability is increased, which means that a faster pace can be maintained for the same effort.
2. IMF and limb blood flow stealing: In order to understand how IMF leads to limb blood flow stealing, we need to understand a little of how blood flow is controlled during exercise. When exercise commences, there is an increased need for oxygen within the contracting muscles, and this is met by increasing blood flow to these muscles. In order to produce the increase in blood flow, the output of the heart must increase, which it does by increasing both the rate and volume of each heart beat.
As exercise progresses, the blood vessels in the working muscles open up (dilate) in response to local factors produced by the exercising muscle. However, during very intense exercise, especially in the heat, the capacity of the heart to pump blood is not sufficient to maintain blood flow to all of the organs of the body, as well as the skin (to dissipate heat) and working muscles (limbs and breathing muscles). So control centres in the brain restrict blood flow to non-essential organs such as the stomach and intestines in order to ensure that the working muscles, skin and the brain continue to be adequately supplied (this is why gastrointenstinal problems sometimes arise during or following exercise).
The flow of blood to other organs is reduced by causing constriction (narrowing) of the blood vessels supplying them; this narrowing reduces blood flow. Unfortunately, there is also a small amount of constriction in the working muscles too, but this is mostly counteracted by the local metabolic factors that induce dilatation, so the net effect is a small amount of constriction (smaller than in the non-essential organs). This tactic is all 'fine and dandy', because the limbs are still getting pretty much what they need. The problem arises when the inspiratory muscles begin to fatigue.
When any muscle works intensely, and with a sub-optimal blood supply, metabolites accumulate inside it. These help to keep the blood vessels open, but they also contribute to failure of muscle contraction (muscle fatigue); the metabolites also stimulate nerve receptors, which in turn trigger a protective reflex.
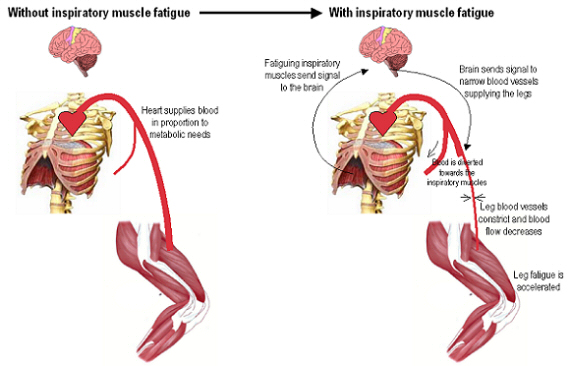
It's this reflex that causes the problems for the exercising limbs, because it induces a much more powerful constriction of the blood vessels (see Figure 2). The reflex is so powerful that it is able to over-ride the local dilating effect of metabolites within the working muscles; the net result now is a reduction in limb blood flow. What happens to the blood that was going to limbs? Its diverted to the inspiratory muscles, in a Robin Hood style ambush that ensures that the 'poor' inspiratory muscles get what they need.
This reflex has two benefits from the viewpoint of the inspiratory muscles; firstly (and obviously), it ensures that they get more blood and oxygen (protecting their vital function); secondly (less obviously), by restricting blood flow the working limbs, the supply of oxygen and removal of metabolic by-products is impaired, which leads to an enforced decrease in exercise intensity (or even cessation), which reduces the breathing demand.
Don't worry if you didn't follow all of the physiology, the only thing you need to know is that when the going gets tough, your inspiratory muscles steal blood from your legs, and that slows you down!
In a recent study from my laboratory, we've shown that IMF makes limb fatigue occur more rapidly; this is because of its effects upon blood flow, but we've also shown that POWERbreathe® training prevents the blood flow stealing reflex from being activated16. Preventing the reflex from being activated also prevents the premature limb fatigue. This helps to explain how POWERbreathe® training improves performance; we believe that the enhanced inspiratory muscle strength, power and fatigue resistance leads to an abolition, or delay in the activation of the blood flow stealing reflex.
Summary
To summarise, we know that rowing induces inspiratory muscle fatigue (IMF), and we also know that IMF is bad news for performance from a number of standpoints -
- IMF leads to a breakdown of breathing and stroke entrainment
- Failure to keep breathing and stroke rhythm entrained leads to a compromise of the structural stability of the trunk, which impairs force transmission and increases the risk of injury
- IMF makes exercise feel harder, reducing the ability to maintain a given pace
- IMF leads to blood flow being diverted away from exercising limbs, accelerating limb fatigue and impairing performance
Take home messages
- Its vital that breathing and stroke rate are entrained during rowing, so spend time working on a breathing strategy that works for you, but try to ensure that its one that results in having a reasonable amount of air in your lungs at the catch
- Work on resisting the urge to allow your breathing to 'run away with you' at the end of a hard piece - maintain discipline and control over your breathing at all times
- Give yourself a 'fighting' chance of achieving breathing discipline by preventing IMF from occurring - do some POWERbreathe® training
References
- Harms CA, Wetter TJ, St Croix CM, Pegelow DF, Dempsey JA. Effects of respiratory muscle work on exercise performance. J Appl Physiol. 2000;89(1):131-8.
- Dempsey JA, Romer L, Rodman J, Miller J, Smith C. Consequences of exercise-induced respiratory muscle work. Respir Physiol Neurobiol. 2006 Apr 28;151(2-3):242-50.
- Steinacker JM, Both M, Whipp BJ. Pulmonary mechanics and entrainment of respiration and stroke rate during rowing. Int J Sports Med. 1993 Sep;14 Suppl 1:S15-9.
- Volianitis S, McConnell AK, Koutedakis Y, McNaughton L, Backx K, Jones DA. Inspiratory muscle training improves rowing performance. Med Sci Sports Exerc. 2001;33(5):803-9.
- Griffiths LA, McConnell AK. The influence of inspiratory and expiratory muscle training upon rowing performance. Eur J Appl Physiol. 2007 Mar;99(5):457-66.
- Loke J, Mahler DA, Virgulto JA. Respiratory muscle fatigue after marathon running. J Appl Physiol. 1982;52:821-4.
- Chevrolet JC, Tschopp JM, Blanc Y, Rochat T, Junod AF. Alterations in inspiratory and leg muscle force and recovery pattern after a marathon. Med Sci Sports Exerc. 1993;25(4):501-7.
- Ker JA, Schultz CM. Respiratory muscle fatigue after an ultra-marathon measured as inspiratory task failure. Int J Sports Med. 1996;17(7):493-6.
- Hill NS, Jacoby C, Farber HW. Effect of an endurance triathlon on pulmonary function. Med Sci Sports Exerc. 1991 Nov;23(11):1260-4.
- Romer LM, McConnell AK, Jones DA. Inspiratory muscle fatigue in trained cyclists: effects of inspiratory muscle training. Med Sci Sports Exerc. 2002 May;34(5):785-92.
- Lomax ME, McConnell AK. Inspiratory muscle fatigue in swimmers after a single 200 m swim. J Sports Sci. 2003 Aug;21(8):659-64.
- Sharpe GR, Hamer M, Caine MP, McConnell AK. Respiratory muscle fatigue during and following a sprint triathlon in humans. J Physiol. 1996:165P.
- Hodges PW, Heijnen I, Gandevia SC. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J Physiol. 2001 Dec 15;537(Pt 3):999-1008.
- Mador MJ, Acevedo FA. Effect of respiratory muscle fatigue on subsequent exercise performance. J Appl Physiol. 1991;70:2059-65.
- Romer LM, McConnell AK, Jones DA. Effects of inspiratory muscle training on time-trial performance in trained cyclists. J Sports Sci. 2002 Jul;20(7):547-62.
- McConnell AK, Lomax M. The influence of inspiratory muscle work history and specific inspiratory muscle training upon human limb muscle fatigue. J Physiol. 2006 Sep 14.